Primary Care, Twelve Steps, and the HIAI–DRT Bridge
Clinical Excerpt (Primary Care Context)
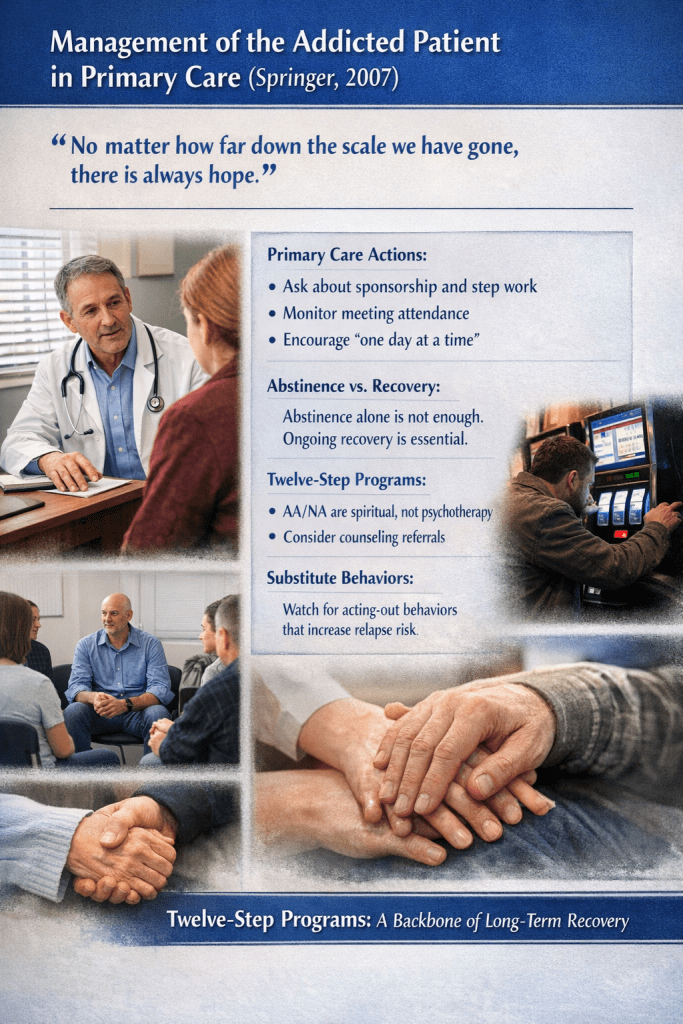
The following excerpt is reproduced from Pomm, H.A., & Pomm, R.M., Management of the Addicted Patient in Primary Care (Springer, 2007), and is presented here to situate Twelve-Step engagement as a recognised medical intervention within primary care.
“No matter how far down the scale we have gone, there is always hope.”
There are few things as gratifying and moving as watching your addicted patient finally grasp the idea of recovery and begin to blossom in every area of his or her life.
When working with patients involved in a Twelve Step program, such as Alcoholics Anonymous or Narcotics Anonymous, physicians are encouraged to ask whether patients have a sponsor, whether they are working the steps, and how often they attend meetings.
It is generally felt in the treatment community that patients who are abstinent but not working a recovery program remain clinically vulnerable.
AA and other Twelve Step programs are spiritual, not religious, and are not psychotherapy. Referral to a therapist familiar with addiction and recovery issues may be appropriate in addition to Twelve Step participation.
Patients should be reminded to take recovery one day at a time, as thinking in lifetime terms can feel overwhelming and counter-productive in early recovery.
Even in recovery, patients may engage in substitute or “acting-out” behaviours that activate similar neurophysiological reward pathways and increase relapse risk.
In our experience, Twelve Step programs have proven to be the backbone of long-term recovery—long after detoxification and formal treatment have ended.
Source: Pomm et al., Management of the Addicted Patient in Primary Care, Springer, 2007.
In clinical reality, addiction is not “solved” in detox. It is stewarded—over time—inside real lives, real bodies, and real follow-up. What struck me reading Management of the Addicted Patient in Primary Care is how plainly it frames the primary care clinician’s role: not as a replacement therapist, but as a steady medical hand who keeps recovery practices in view, visit after visit.
Primary care as steward of recovery
A clinical snapshot from Management of the Addicted Patient in Primary Care (Springer, 2007): hope held in structure, continuity over crisis, recovery observed in lived behaviour—not declared intention.
The medical stance: hope, structure, follow-up
The tone is both sober and kind. The excerpt opens with hope, then moves immediately into concrete, primary-care actions—simple questions that function as clinical orienting instruments: sponsorship, step work, meeting rhythm, and what the patient is actually doing between appointments.
The message is clear: recovery is observable in behaviour, not merely declared in intention.
AA/NA as recovery architecture (not psychotherapy)
Pomm & Pomm name a boundary that matters for safe care. Twelve-Step fellowship is not a substitute for therapy. That single clarification protects patients, clinicians, and the fellowship itself from misuse or confusion of roles.
DRT language: from abstinence to recovery (the difference that shows)
In DRT terms, abstinence can be a necessary pause, but recovery is a lived re-patterning. Without structure, a person can remain internally driven, brittle, and relapse-prone even while substance-free.
What looks like “non-compliance” may be the organism’s attempt to re-route pressure through familiar channels. The clinical task is not to shame the channel, but to help build a new one that can carry load without rupture.
The primary care micro-interventions (small questions with big leverage)
- sponsorship (including temporary sponsorship),
- active engagement with the Twelve Steps,
- meeting frequency and rhythm,
- the patient’s subjective experience of meetings.
The power here is not ideology—it is continuity. In systems where addicted patients are often treated episodically, continuity itself becomes a form of medicine.
“One day at a time” as nervous-system realism
This is not a slogan. It is a time-horizon intervention. “Just today” restores scale, reduces overwhelm, and allows the nervous system to stand down.
Acting-out substitutions: relapse risk wearing new clothes
Substitute behaviours—gambling, sexual acting out, compulsive work, overspending—are not moral failures. They are signals that reward circuitry remains recruitable. Skilled curiosity, not surprise, is the appropriate clinical stance.
HIAI framing: the qalam that serves the same Source
HIAI—Human–AI Intelligence—is our USP: the qalam of human and artificial intelligence, the Unseen helping the Seen, both answering to the same Source. It allows translation, clarity, and continuity—without pretending we can mechanise conscience, awakening, or grace.
Primary care can remain primary care. Fellowship can remain fellowship. Therapy can remain therapy. And the patient can remain—first and last—a person.