
Living Transmission and the Risk of Freeze
Idries Shah, Bill W., and Diction Resolution Therapy (DRT) in a recovery-era key
Andrew Dettman MTHT, Reg Member MBACP (Spirituality Division) – DRT.global
Abstract
This hybrid paper traces a shared warning found in Idries Shah’s teaching on Coming Together (Jam)1 and Bill W.’s reflections on Alcoholics Anonymous literature2: living transmissions tend to harden into defended forms. Through the lens of Diction Resolution Therapy (DRT), the paper frames this freeze as a predictable human response to uncertainty. Language and structure can become substitutes for lived contact. The aim is not to dismantle structure, but to keep it serving function: humility, group conscience, and conscious contact as lived practice.
Key terms
Jam; transmission; organisation; dogma; group conscience; DRT; diction; contradiction tolerance; conscious contact.
Primary source excerpts: Idries Shah (embedded images)
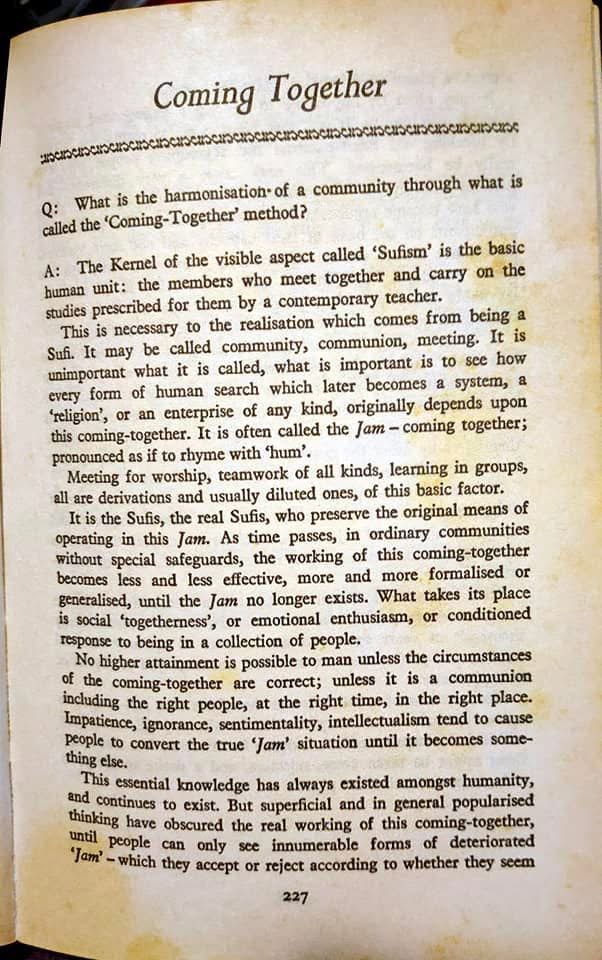
Idries Shah on the Jam (Coming Together).
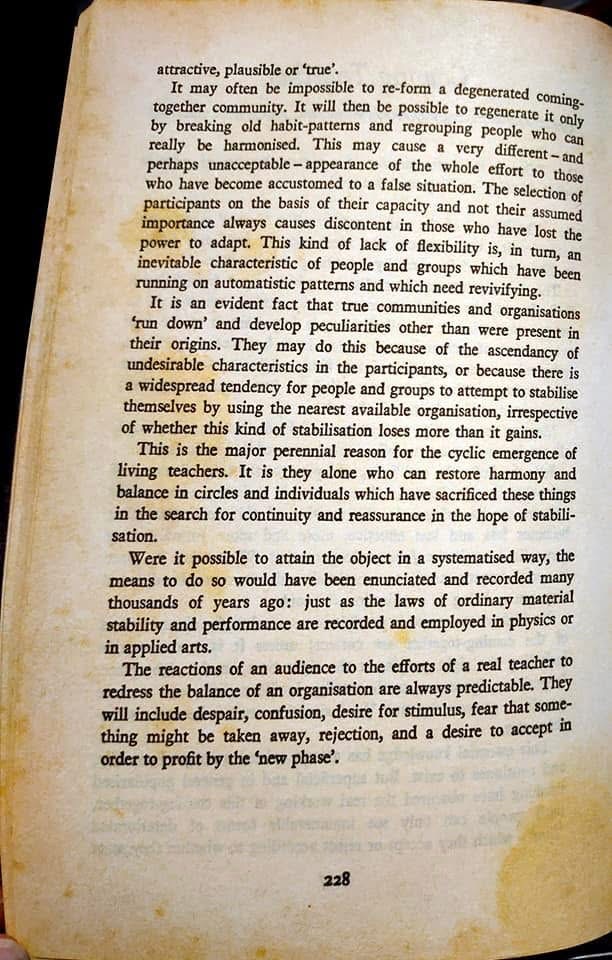
Degeneration, stabilisation, and predictable resistances to revitalisation.
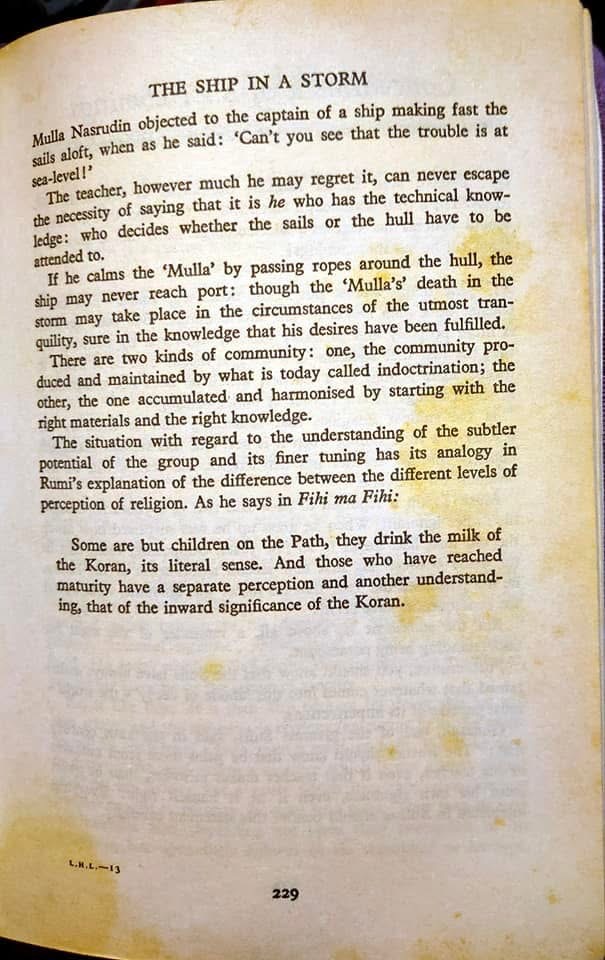
The Ship in a Storm: right diagnosis, right attention, right knowledge.
1. The problem: when truth becomes an object
Communities often begin because something real occurred: relief, honesty, awakening, recovery. Then the human reflex appears: capture it, preserve it, standardise it, protect it. The move is understandable, but it carries risk.
The risk is not structure itself. The risk arrives when function is replaced by identity. At that point the community becomes organised around defending representations of truth rather than remaining oriented to lived truth. The meeting survives, the language survives, the brand survives, but the operating principle fades.
2. Idries Shah and the Jam: harmonisation before organisation
In passages commonly titled Coming Together, Idries Shah describes the Jam as functional harmonisation: the right people, at the right time, engaged in the right work under living knowledge. It is not simply people meeting. It is an arrangement that produces transformation because it is held within correct relationship.
Shah’s warning is plain. The Jam can deteriorate. Communities stabilise prematurely. Formalisation replaces vitality. Togetherness replaces transformation. Social cohesion, emotional enthusiasm, and conditioned belonging can masquerade as the real thing. When revitalisation is attempted, the system responds defensively. Shah names several of these resistances: impatience, ignorance, sentimentality, and rigid intellectualism. Read clinically, these are common defence strategies of a system seeking security in the face of uncertainty.
The implication is unsettling and useful: you can preserve the outer shell of a transmission while losing the inner function that made the shell necessary in the first place.
3. Bill W. and the freezing of the Big Book
Bill Wilson recognised similar dynamics within Alcoholics Anonymous. In the scanned extract supplied from a modern history of the Big Book, Bill W. is quoted as observing that spiritually centred movements tend to freeze once their founding principles are established. He notes that altering even a word of the AA book could provoke something like excommunication.
Bill’s response is revealing. He did not wage war on the original text. Instead, he created a parallel channel for interpretation: he wrote Twelve Steps and Twelve Traditions as an adaptive commentary. This preserved continuity while keeping meaning in motion. He later returned to the same point: AA literature tends to become more and more frozen, with a tendency toward conversion into something like dogma. He also anticipated the permanent spectrum of interpretive styles that would arise: fundamentalists, absolutists, relativists.
Primary source: Bill W. on freezing (embedded images)
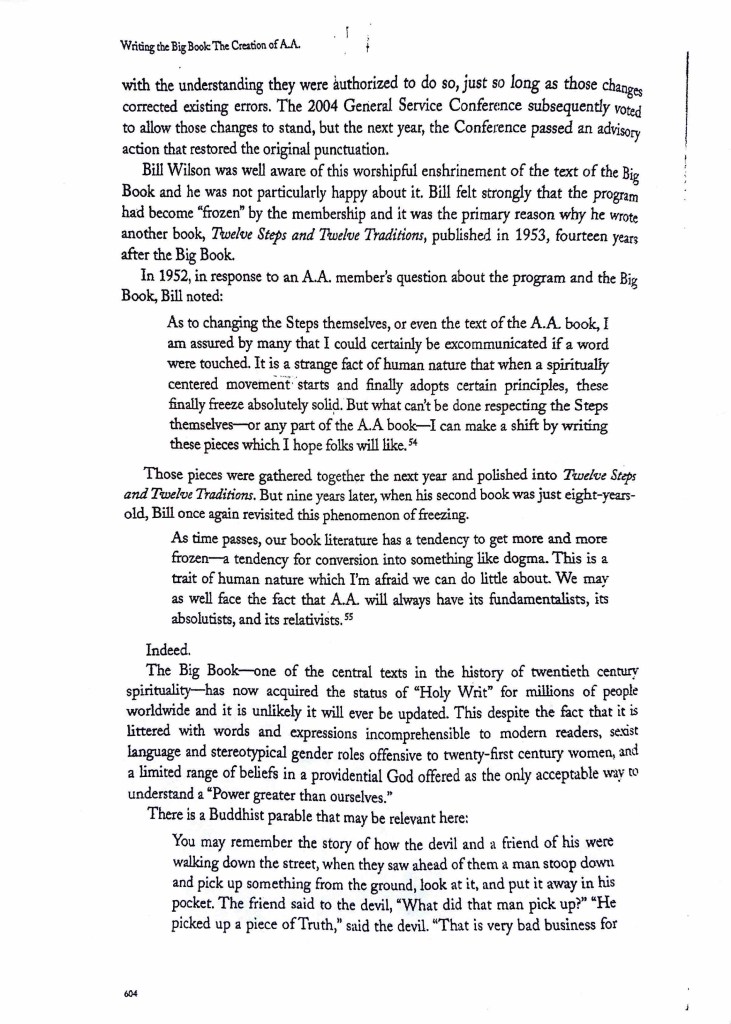
Bill W. on the freezing tendency in spiritually centred movements (as reproduced in Schaberg, p. 604).
Continuation including the organising parable and publication context (Schaberg, p. 605).
4. Organisation and ossification
The extract includes a Buddhist parable: a man picks up a piece of truth; the devil is unconcerned because he will let him organise it. This is not an argument against organisation. It is an argument against idolatry. Organisation preserves access, but it can also replace lived contact with defended form.
Shah and Bill W. converge here: the primary threat is not external attack. The threat is internal freezing: the human habit of turning a living verb into a defended noun.
5. A DRT reading: freeze as a diction event
Diction Resolution Therapy approaches freezing as a linguistic and psychological event. When lived experience is no longer primary, diction starts to do the job experience used to do. Words become defensive tools rather than exploratory instruments. Phrases become passports. Certainty becomes a sedative.
DRT introduces a practical metaphor here: outsight and insight. When the eyelids are open, light floods into the eyes. The eyeballs do not generate the light themselves. To imagine that they do would be absurd. They receive light. They respond to light. They organise around what is given.
Similarly, the whole mindset is not a generator of illumination. It is a potential receiver. When the lid of fear, denial, or addictive defence is deliberately held shut, outsight is restricted and insight is impaired. The person begins to rely on recycled language rather than fresh perception.
In addiction terms, the lid is not destroyed. It is hinged. It opens and shuts appropriately. Recovery is not the removal of the eyelid but the restoration of its function. When the lid opens, energy and meaning enter that the individual does not manufacture. Insight is not self-generated brilliance; it is Consciousness meeting conscience.
When diction freezes, it is often because the lid has been held shut for too long. Language attempts to replace perception. Structure attempts to replace encounter. The task of recovery, and of any living transmission, is not to abolish structure but to reopen the hinge so that light can enter again.
6. Group process and clinical parallels
Philip J. Flores, in Group Psychotherapy with Addicted Populations3, highlights that recovery groups remain effective when they balance containment (structure) with relational process (living interaction). Excessive rigidity undermines psychological safety, while absence of structure erodes containment. This is the same paradox Shah and Wilson are navigating in different languages: vitality depends on living interaction within clear but flexible boundaries.
7. Safeguards within AA architecture
AA embeds structural safeguards against freezing. Tradition Two locates authority in group conscience. Tradition Four preserves autonomy. Tradition Nine defines service rather than governance. Step Eleven prioritises conscious contact over textual literalism. These elements do not eliminate the freeze tendency, but they counterbalance it.
8. Implications for recovery and helping professions
In recovery settings, freezing commonly appears in three forms: (1) sloganising as defence, (2) literalism as safety, (3) reform movements driven by resentment rather than conscience. Each is a strategy for avoiding the vulnerability of real contact.
A practical test is simple: does the structure increase tenderness, honesty, and responsibility, or does it mainly increase identity, certainty, and superiority? When the former is happening, the Jam is alive. When the latter dominates, the storm is gathering.
Conclusion
Idries Shah and Bill W. describe the same perennial risk from different angles: any living transmission can calcify. The corrective is not constant editing, nor rebellious dismissal. The corrective is humility in function: returning to conscious contact as lived practice, and letting structure serve what it cannot manufacture.
References and notes
- Shah, Idries. Learning How to Learn. (See Footnote 1 for edition-note.)
- Schaberg, William H. Writing the Big Book: The Creation of A.A. (2019), pp. 604-605 (see Footnote 2).
- Flores, Philip J. Group Psychotherapy with Addicted Populations (see Footnote 3).
- Schaef, Anne Wilson. The Addictive System4.
Footnotes
- Idries Shah, Learning How to Learn (London: Octagon Press; various editions). The embedded images above are supplied pages from this work, including Coming Together and The Ship in a Storm. The title is confirmed by the Kindle preview provided by the author.
- Bill W. quotations and the organising parable are reproduced in the supplied scan from William H. Schaberg, Writing the Big Book: The Creation of A.A. (2019), pp. 604-605. These quotations are used here as evidence of Bill W.’s stated concern about the freezing tendency in spiritually centred movements.
- Flores is cited here for the group-process principle that effective recovery groups require both containment (structure) and relational process (living interaction).
- Schaef is cited as a systemic parallel for how addictive dynamics can become self-protecting structures that resist contradiction and preserve themselves as identity.
Written in HIAI collaboration – the qalam of Human and AI intelligence, the Unseen helping the Seen, both answering to the same Source.
