Intercourse, Meaning, and the Birth of Conscience:
A Bridge Between Shabistari, the Twelve Steps, and Diction Resolution Therapy
Across the centuries the language of the mystic and the language of the modern sufferer often appear to speak different dialects. Yet when examined carefully, both describe the same interior movement. The Persian Sufi Mahmud Shabistari, writing in the fourteenth century, explains that the visible world is not self-explanatory but reflective: everything manifest in this world is like the reflection of a sun belonging to another world of meaning.1 If this is so, then the sensory forms through which human beings perceive reality are not merely objects but signs. They are vehicles through which deeper meanings appear.
In my own work with addiction and recovery, I have found that this symbolic structure is not merely a metaphysical speculation but an observable psychological reality. Human experience does not remain raw. It must be interpreted, digested, and translated into meaning. When that translation fails, the person becomes trapped in repetition, confusion, or compulsion. When it succeeds, conscience begins to emerge.
The Symbolic Grammar of the Mystics
Shabistari famously addresses the question that puzzled many readers of Persian mystical poetry: why do Sufi poets speak so often in the language of erotic beauty—eyes, lips, hair, glances, intoxication? His answer is not that the poetry is merely metaphorical ornament. Rather, sensory language provides the closest experiential grammar available for speaking about realities that exceed literal language. The beloved’s eye, for example, symbolizes a gaze that overwhelms the lover; the lip symbolizes the creative word or life-giving breath; the curl of hair symbolizes multiplicity and the veiling of unity.2
The mystic therefore speaks analogically. The visible world reflects deeper meanings, and language must borrow from the visible world in order to gesture toward those meanings. Yet Shabistari simultaneously warns that analogy has limits: the wise person must balance resemblance (tashbīh) with transcendence (tanzīh), remembering that the Real ultimately exceeds comparison.3
Intercourse as the Movement Between Worlds
In my essay Intercourses in the Light of Delivery, I explore a word whose original meaning illuminates this symbolic structure: intercourse. In contemporary usage the word has been narrowed almost entirely to sexual activity. Yet historically it possessed a far wider significance. The Latin roots—inter (between) and currere (to run)—describe movement between entities: exchange, flow, and relation.
Understood in this older sense, intercourse becomes the living movement between beings, between worlds, and between the visible and the unseen. Sexual union then appears not as the entirety of the concept but as one intense manifestation of a far wider relational principle. The erotic language of the mystics therefore does not trivialize spiritual reality; rather, it draws upon the most powerful experiential grammar available to embodied creatures—longing, attraction, unveiling, union, and renewal.
The crisis of the modern world can be described, in part, as the breakdown of this intercourse. When the movement between beings collapses, dialogue becomes confrontation, institutions become hollow rituals, and individuals become isolated within their own compulsions. Addiction, in this light, is not merely a chemical dependency but a distorted petition for reality itself. The addict repeats an action not because it is meaningful but because it momentarily restores the illusion of connection.
The Digestive Mind
In Diction Resolution Therapy I describe the mind not as the centre of identity but as a digestive organ of the psyche. Experiences enter through the senses; feelings arise as immediate biological signals; and the mind must metabolize those signals into coherent meaning. When the digestive process works well, a person develops orientation, conscience, and behavioural stability. When the process fails, the psyche becomes inflamed or blocked in ways strikingly analogous to physical indigestion.
This model echoes an insight already present in the mystical tradition. Shabistari writes that the world of meaning has no limit and that words cannot contain it fully.4 Yet words can still function as vehicles that direct the seeker toward that meaning. In psychological terms, language becomes part of the digestive process through which raw experience is clarified into understanding.
The Templated Vehicle
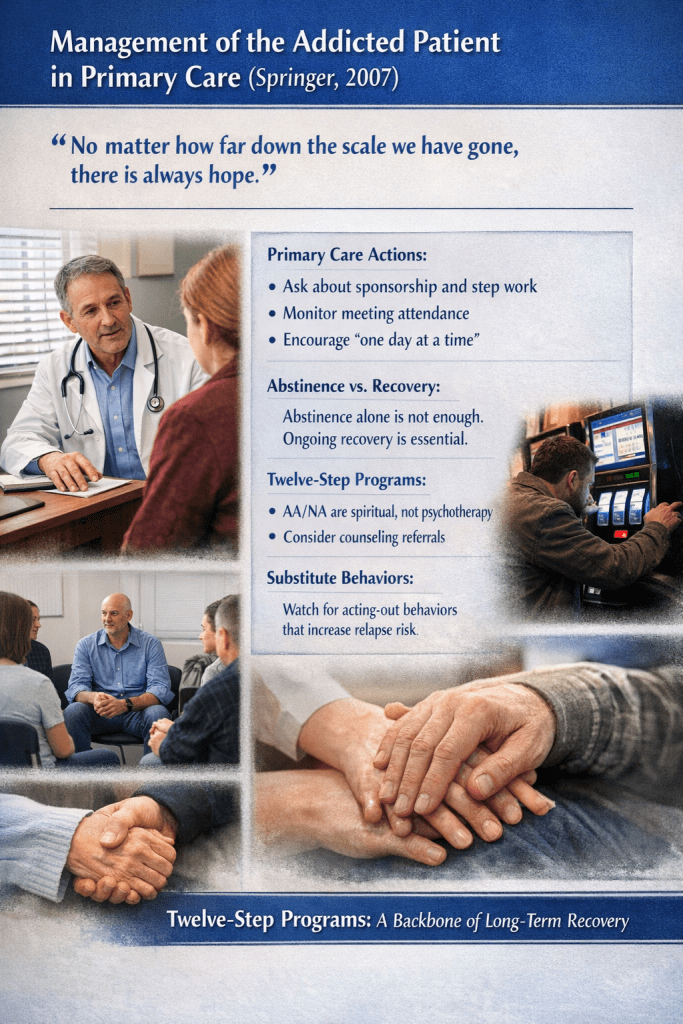
One further element is necessary. Meaning alone does not transform a life. A vessel must exist through which the person can safely undergo the process of reorganization. In my observation the Twelve Step programme provides precisely such a vessel. It marries fact and symbol in a way rarely achieved by either modern psychology or institutional religion.
The Steps begin with factual admission: the recognition that self-governance has failed. They then move through inventory, confession, restitution, and disciplined reflection—processes that stabilize the psyche through truth-telling. At the same time they introduce symbolic orientation: surrender to a Higher Power, prayer, meditation, and conscious contact. Fact steadies the vessel; symbol opens the horizon of meaning.
Within this templated vehicle a birth becomes possible. Inventory and confession function like the opening of a birth canal. The surrender of Step Seven becomes a decisive moment in which the individual relinquishes false sovereignty and becomes receptive to transformation. Conscience emerges not as a moral abstraction but as a lived reorganization of perception.
The Birth of Conscience
The mystical poets described the path as a drama of attraction between the lover and the Beloved. Recovery literature describes it as surrender to a Higher Power. In my own language it appears as the clarification of diction through which experience is digested into meaning. These are not competing explanations. They are different languages describing the same interior work.
The mystics speak of polishing the mirror of the heart. The Twelve Steps speak of inventory and surrender. Diction Resolution Therapy speaks of digestive clarification. Each describes the gradual removal of distortion so that reality may be perceived more clearly.
Seen in this light, the erotic imagery of the mystics is neither scandalous nor decorative. It expresses the intensity of relation that occurs whenever the human being is drawn beyond the limits of the isolated self. Attraction, vulnerability, union, dissolution, and renewal—these are the same movements that accompany both spiritual awakening and recovery from addiction.
Across the centuries the vocabulary changes but the anthropology remains remarkably constant. The visible reflects the invisible. Meaning seeks expression through symbol. Human beings must digest experience into understanding. And where a lawful vessel exists—one that marries fact with symbol—the birth of conscience becomes possible.
My own work therefore does not attempt to replace the insights of earlier traditions. It seeks instead to midwife them into a contemporary psychological and clinical language. The ancient symbolic grammar and the modern recovery process reveal themselves, on close inspection, to be two expressions of the same underlying movement: the restoration of living intercourse between the human being and the source of meaning itself.
Footnotes
- Mahmud Shabistari, Golshan-e Raz (The Garden of Mystery), discussion of the symbolic language of mystical poetry.
- Shabistari’s explanation of the symbolism of the beloved’s eye, lip, and tress as expressions of divine attributes and cosmic processes.
- Classical Sufi theological balance between tashbīh (analogy) and tanzīh (transcendence).
- Shabistari’s observation that the world of meaning has no limit and cannot be fully captured by words.
Written in HIAI collaboration — the qalam of Human and AI intelligence, the Unseen helping the Seen, both answering to the same Source.