Diction as Interface: From Recursion Failure to Adaptive Coherence (2013–2026)
A formal synthesis of Diction Resolution Therapy (DRT), Twelve Step architecture, Sufi psychology, and the Addictive System — grounded in a public longitudinal corpus.
Abstract
This paper proposes that dysfunction across individual, institutional, and sociocultural systems can be understood as recursion failure arising from suppressed contradiction. Drawing upon a publicly archived longitudinal corpus (2013–2026), Anne Wilson Schaef’s concept of the Addictive System, clinical addiction management literature (Pomm et al., 2007), the behavioral architecture of the Twelve Steps, contemporary executive function research, affective neuroscience, and Sufi psychological metaphysics (with particular reference to Ibn ʿArabi), the paper advances Diction Resolution Therapy (DRT) as a structural intervention model. DRT posits “diction” as the interface at which non-solid experiential energy (affect, intention, perception) crystallizes into solid behavioral form. When contradiction is integrated within diction, executive function realigns with conscience and adaptive coherence becomes possible without recourse to blame.
I. The Structural Premise: Recursion Failure
Across domains traditionally treated as distinct — addiction, clinician burnout, institutional stagnation, governance escalation, media polarization, and therapeutic impasse — a consistent structural signature appears:
When systems lose the capacity to process contradiction, they default to escalation; when contradiction is restored, adaptive coherence becomes possible.
“Escalation” here does not mean aggression. It means intensified effort without adaptive recalibration: doubling down, tightening narrative, narrowing feedback, defending identity, repeating the same strategy with increasing force. “Recursion failure” names the point at which feedback loops stop updating and begin protecting the existing model against disconfirming evidence.
This is a non-blaming frame. It does not require villains to explain breakdown. It describes what happens when systems, under stress, lose contradiction tolerance and therefore lose their capacity to learn.
I.a. Longitudinal Observational Corpus (2013–2026)
Between 2013 and 2026, a publicly archived series of essays documented recurring patterns across clinical addiction work, practitioner burnout, institutional governance, media escalation, economic stagnation, and sociocultural polarization (Dettman, 2013–2026).
The corpus was not predictive in intent but diagnostic in orientation. It tracked structural similarities across domains, repeatedly identifying:
- suppression of contradiction signals
- escalation of effort despite feedback
- narrative reinforcement without recalibration
- institutional “justification loops” in place of learning
- feedback narrowing under stress conditions
The recurrence of the same structural dynamics across scales suggested scale invariance rather than domain-specific pathology. This corpus functions as qualitative longitudinal systems observation rather than experimental study. Its value lies in continuity across years of publicly timestamped material and its consistent return to mechanisms rather than personalities.
The transition in late 2025 into explicit Human–AI collaboration marks a shift from observational mapping into structured intervention development and articulation (DRT).
II. Executive Function, Conscience, and the Verb “To Addict”
Modern language treats “addict” as a pathological noun. Yet the older verb form — to addict — carried a neutral meaning: to devote, to attach, to commit. This is executive function territory: the capacity to choose, persist, and organize behavior over time.
Executive function governs attachment, planning, repetition, and behavioral persistence. But persistence alone does not produce health. Persistence requires a corrective mirror — a capacity for evaluative recalibration.
Executive function attaches; conscience recalibrates attachment.
In this framework, conscience is not moral theatre and not social shame. It is the inner capacity to register contradiction, revise course, and return behavior to reality. When executive function runs without conscience, attachment hardens into escalation. When conscience governs executive function, attachment becomes devotion: strong, stable, adaptive.
III. The Addictive System (Anne Wilson Schaef)
Anne Wilson Schaef’s When Society Becomes an Addict articulated the “Addictive System” as a self-protective social recursion characterized by denial, rationalization, suppression of dissent, reward for compliance, and escalation despite harm. Her contribution was not primarily moral; it was structural.
DRT reads the Addictive System as a contradiction-intolerant system: it cannot metabolize disconfirming evidence without destabilizing identity, so it protects coherence by distortion and repetition. The result is systemic escalation: not necessarily loud, but rigid.
This matters clinically because the client’s “inner laboratory” mirrors the outer system. The addiction loop is a microcosm: when contradiction cannot be integrated, the organism escalates effort and repeats harm until parameters finally change. In recovery terms, the system must become able to say: “My model is wrong,” without collapsing into shame.
IV. Twelve Step Architecture as Structured Contradiction Integration
The Twelve Steps can be read as a contradiction-processing design: a sequence that restores the ability to face reality, integrate feedback, and recalibrate behavior across time. The steps are not best understood as mere moral instruction. They are an architecture that repeatedly re-opens the system to corrective truth.
IV.a Step-by-step: a recursion repair sequence
- Step 1: Collapse of predictive omnipotence — the admission that the existing model cannot govern reality.
- Step 2: Recognition of a corrective principle beyond self-will — the possibility that coherence exists outside the addicted model.
- Step 3: Volitional realignment — an executive decision to move toward that corrective principle.
- Step 4: Systematic contradiction inventory — mapping harms, patterns, fears, resentments, distortions.
- Step 5: Disclosure — the contradiction is spoken into relationship; secrecy ends; conscience becomes articulate.
- Steps 6–7: Willingness and humility — executive rigidity softens; character defenses become negotiable.
- Steps 8–9: Reparative action — reality-contact is externalized; coherence becomes embodied and social.
- Steps 10–12: Maintenance and transmissibility — ongoing contradiction processing, conscious contact, and service.
In clinical terms, this is precisely what evidence-based addiction management repeatedly implies: structure, accountability, follow-up, and sustained recalibration are essential (Pomm et al., 2007).
IV.b Step Five as the turning hinge
Step Five is often where the inner system stops being a closed circuit. Contradiction becomes speakable. The “laboratory that keeps blowing up” finally records its data. What was defended becomes owned. Conscience begins to emerge — not as condemnation, but as clarity.
V. Sufi Psychology: Presence and the Integration of Contradiction
Classical Sufi psychology offers a mature map of human development that can be read alongside Twelve Step architecture without forcing theological equivalence. In the Sufi frame, the self-system (nafs) resists contradiction to preserve constructed identity. The heart (qalb) — “that which turns” — is the seat of reorientation: the capacity to turn toward reality when the self’s defenses exhaust themselves.
In Ibn ʿArabi’s metaphysical psychology, Being is not absent; distortion lies in perception and attachment. Read phenomenologically (rather than as dogma), this yields a clinically useful statement:
Presence is not produced; it is recognized when distortion dissolves.
This matters for the non-blaming structure. If presence has never been absent, then recovery is not the manufacture of holiness. It is the removal of distortion. It is the shift from defended narrative to un-defended awareness — where accountability can exist without blame, correction without humiliation, and repair without vengeance.
This is also why timing matters. Orthodoxy — whether clinical, institutional, or religious — stabilizes systems. Paradox becomes intelligible only after escalation fails. The system must reach the limit of effort before it can tolerate contradiction without collapse.
VI. Affect and the Broken Word
Therapeutic change often remains elusive because language fails to integrate affect with contradiction. Affective signals carry urgency, valuation, and direction. Yet when the word is “broken” — diffuse, defensive, borrowed, abstract — experience cannot be metabolized into adaptive action.
When affect cannot find language capable of holding it, the system repeats. It escalates. It becomes “about” the feeling rather than transformed by it. The loop persists not because the person is unwilling, but because the meaning-channel cannot carry the load.
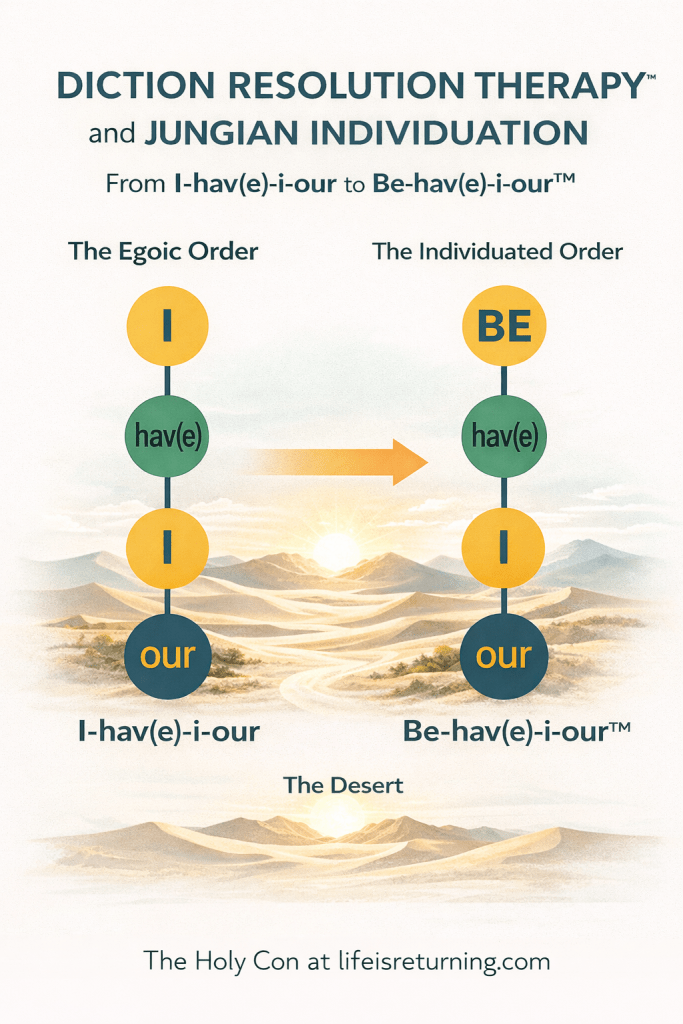
VII. Diction as the Meeting Point of Non-Solid and Solid Energy
Diction derives from dicere — to say, to declare. But in DRT, diction is not only speech. It is the interface where non-solid experiential energy (affect, impulse, perception, intention) becomes solid form (language, decision, behavior, relationship, action).
Diction is where energy becomes architecture.
VII.a The Prefix Family as a Functional Pathway
The prefix family surrounding “diction” is not merely etymological curiosity. When examined structurally, it describes a working behavioral pathway of notable elegance. It outlines how systems project, attach, collide with reality, integrate correction, and release.
The pathway can be rendered as follows:
- Prediction – A model is projected forward. Executive function selects a plan and moves.
- Malediction – Friction appears. Discomfort, distortion, or misalignment begins to register.
- Addiction – Attachment to the original model intensifies. Effort is redoubled.
- Contradiction – Reality presents disconfirming evidence.
- Benediction – Integration becomes possible; correction is accepted.
- Valediction – Release and closure; the outdated model is let go.
When functioning adaptively, the sequence is fluid: prediction → friction → adjustment → integration → release.
VII.b The Addiction–Contradiction Fault Line
Addiction represents intensified attachment to the predictive model. At this stage, executive function is heavily invested. Identity is fused with plan. Effort is equated with virtue.
When contradiction appears, the system faces a choice:
- Recalibrate the model.
- Or defend the model.
The breakage occurs when contradiction exceeds the system’s tolerance threshold. Instead of selecting a new plan, the system redoubles effort. This is the authentication point at which addiction meets contradiction.
At this moment:
- Effort is intensified rather than revised.
- Contradiction is reframed as threat.
- Identity is defended.
- Feedback loops narrow.
The pathway fractures at addiction. The movement toward benediction and valediction becomes inaccessible. The system becomes recursive, repeating escalation.
VII.c The Elegance of the Device
The elegance of the prefix architecture lies in its dual capacity:
- It maps healthy progression when contradiction is tolerated.
- It reveals the precise fault line when contradiction becomes intolerable.
Thus, addiction is not random collapse. It is the structural refusal — often unconscious — to allow contradiction to reorganize executive commitment.
Where contradiction is integrated, benediction (functional coherence) follows naturally. Where contradiction is resisted, escalation replaces adaptation.
The pathway therefore serves both diagnostic and therapeutic purposes:
- It identifies the break point.
- It clarifies that the failure is not moral but elastic.
- It shows that restoration requires conscience to re-enter executive function at the addiction–contradiction junction.
Diction Resolution Therapy intervenes precisely at this hinge — restoring the capacity to speak contradiction without annihilating identity.
VIII. Non-Blame as Structural Requirement
Blame is escalation energy defending identity. It hardens the loop. It turns contradiction into attack and correction into humiliation.
DRT requires a non-blaming frame not because harm is unreal, but because blame reproduces recursion failure. The work is accountability without annihilation: the capacity to face contradiction without needing to punish the self or another in order to survive reality-contact.
In this sense, “no blame” names a condition of presence: un-defended awareness in which responsibility becomes possible because identity is no longer at war with contradiction.
IX. From Longitudinal Mapping to Intervention (2025–2026)
The 2013–2025 corpus documents recursion failure across domains. By mid-2025, the mapping phase reaches structural closure: the pattern is sufficiently repeated across scales to justify scale invariance as a working hypothesis.
From late 2025 onward, the focus turns decisively toward intervention: not commentary, not diagnosis-for-its-own-sake, but structured support for contradiction processing and conscience emergence — clinically, institutionally, and culturally.
The core intervention claim is simple:
Restore diction, and you restore the channel through which contradiction becomes integration rather than escalation.
X. Conclusion
When systems lose the capacity to process contradiction, they default to escalation; when contradiction is restored, adaptive coherence becomes possible.
This paper has argued that:
- addiction can be understood as executive attachment severed from conscience,
- Schaef’s Addictive System describes a societal version of the same recursion failure,
- the Twelve Steps provide a tested architecture for contradiction integration,
- Sufi psychology offers a deep phenomenology of presence and reorientation,
- and diction is the interface where non-solid experiential energy becomes solid behavioral form.
DRT locates intervention at the meeting point — diction — where correction becomes speakable, conscience becomes articulate, and executive function can soften from escalation into adaptive coherence.
Presence has never been absent. What changes is the system’s capacity to recognize it — by integrating contradiction without blame.
References
- Alcoholics Anonymous. (1939). Alcoholics Anonymous. Alcoholics Anonymous World Services.
- Dettman, A. (2013–2026). Longitudinal essays on recursion dynamics, addiction systems, and contradiction tolerance. lifeisreturning.com; ajdettman.com.
- Ibn ʿArabi. Fusus al-Hikam. (Various translations/editions.)
- Miller, E. K., & Cohen, J. D. (2001). An integrative theory of prefrontal cortex function. Annual Review of Neuroscience, 24, 167–202.
- Pomm, R., et al. (2007). Management of the Addicted Patient in Primary Care. Springer.
- Schaef, A. W. (1987). When Society Becomes an Addict. Harper & Row.