The Middle Built
Addiction, Instinct, and the Sanitation of the Soul
“In the beginning was the Word, and the Word was with God, and the Word was God.” The grammar is deliberate. Was. With. Origin and relation. The future is not mentioned. It is not forecast. It is not guaranteed. It appears. Most human beings live suspended between was and will, pulled by memory behind and projection ahead. Regret becomes gravity. Fear becomes anticipation. The present is reduced to a narrow corridor through which the self rushes without ever dwelling. Recovery is the building of a middle. The Twelve Step Programme is not an abstract theology and not a philosophical treatise. It is infrastructure. It is plumbing for the soul.
When the agricultural world became industrial, waterborne diseases exposed the breakdown of outer sanitation. Cholera did not arrive because humanity suddenly became immoral; it arrived because systems had not evolved to handle density. Waste accumulated. Disease followed. Addiction functions similarly in this era. It is the bellwether disease of overstimulation, fragmentation, and unprocessed shame. It exposes the failure of inner sanitation. It reveals what happens when psychic waste is not metabolised. The problem is not instinct. The problem is accumulation.
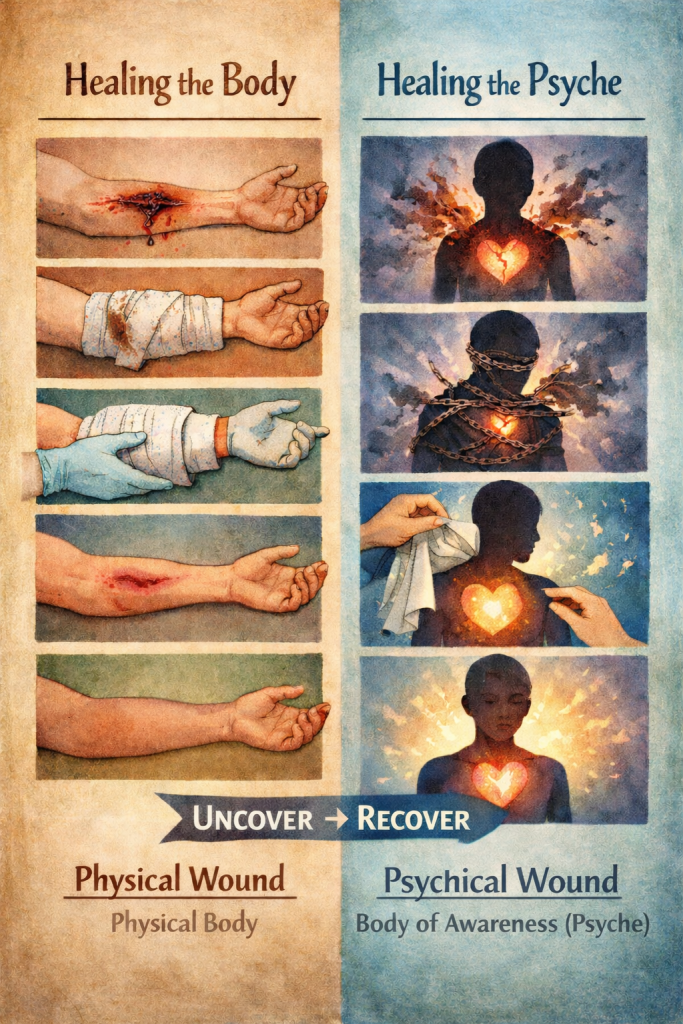
Addiction is not merely about alcohol, substances, or behaviours. It is disordered relationship. Relationship to one’s own story. Relationship to desire. Relationship to fear. Relationship to other people. Relationship to God. “I have a story. It is not who I am.” That sentence marks a decisive shift. The story can be examined without being identical to the self. Once that distinction is made, digestion becomes possible.
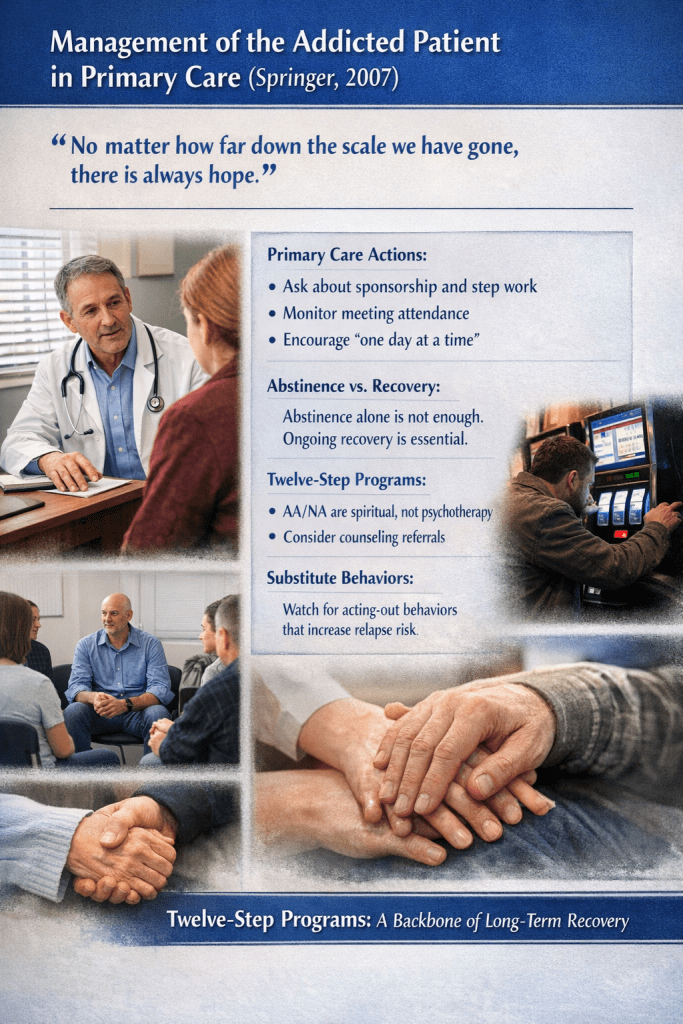
The psyche, when healthy, operates like a digestive organ. Thoughts are not identity; they are movement. They churn experience. They break down what has been swallowed. They extract nourishment and eliminate what no longer serves. When the system is inflamed, peristalsis becomes cramping. Rumination replaces integration. Secrecy replaces elimination. The Twelve Steps introduce a disciplined digestive process: inventory, confession, amends, service. Inventory is chewing. Step Five exposes waste to air. Amends remove toxicity from the relational field. Service restores circulation.
The Big Book does not speak poetically here; it speaks clinically: “If we are not sorry, and our conduct continues to harm others, we are quite sure to drink. We are not theorizing. These are facts out of our experience.” The warning is not about instinct in isolation. It is about conduct. It is about harm. Continued harm corrodes conscience. Corroded conscience produces shame. Shame seeks anaesthesia. Relapse is not mystical punishment; it is emotional consequence.
The sex instinct is addressed directly because it is powerful, intimate, and easily distorted. But the Steps do not condemn sexuality. They confront misuse. Instincts—sexual, social, and security-based—are God-given and good. When unmanaged, they fragment relationship. Fragmented relationship breeds secrecy. Secrecy splits the psyche. Split psyches seek relief. Integration across Eros, Philia, and Agape is not theological ornament; it is behavioural alignment. Desire acknowledged without exploitation. Friendship honoured without manipulation. Love enacted without transaction.
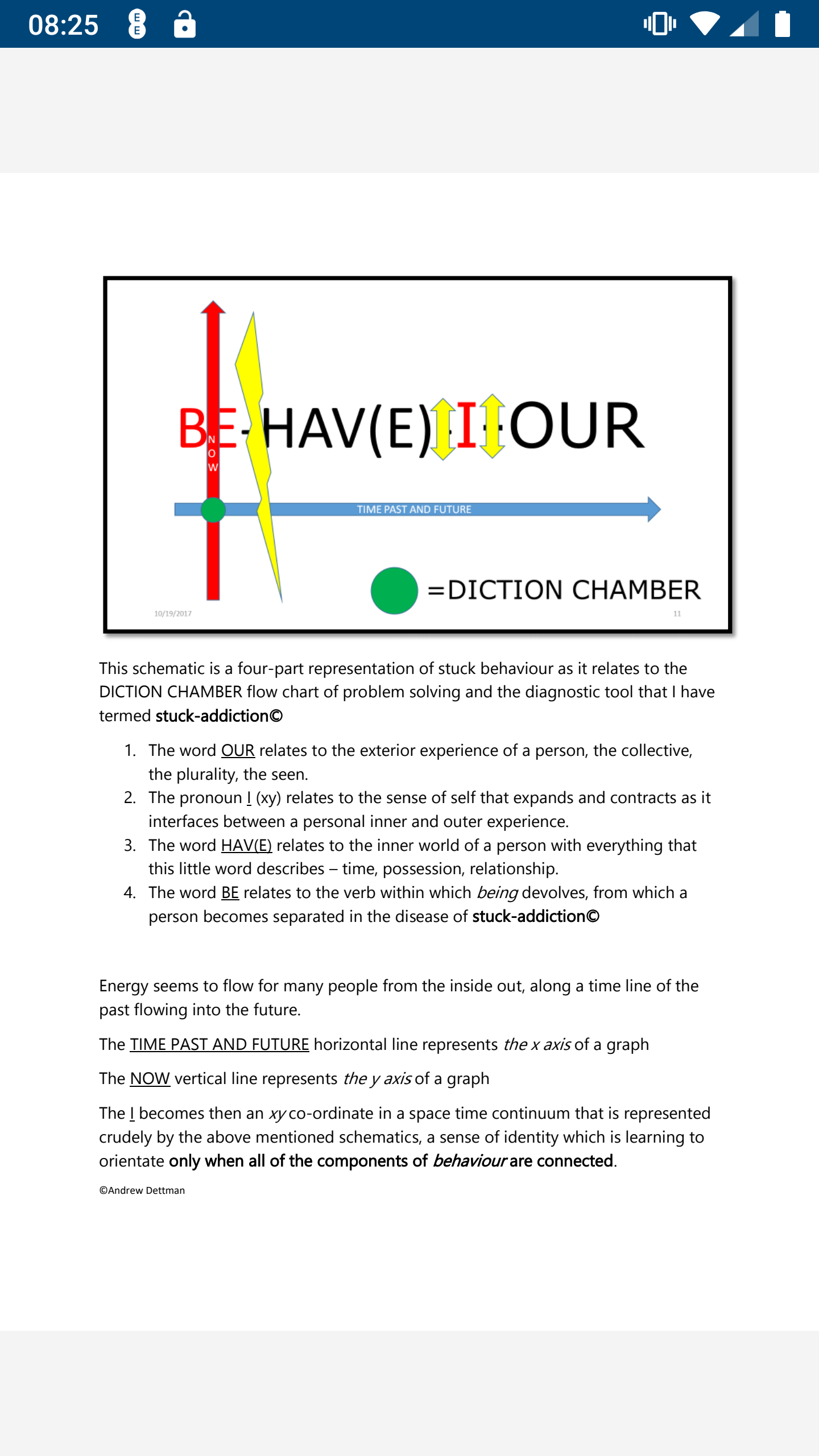
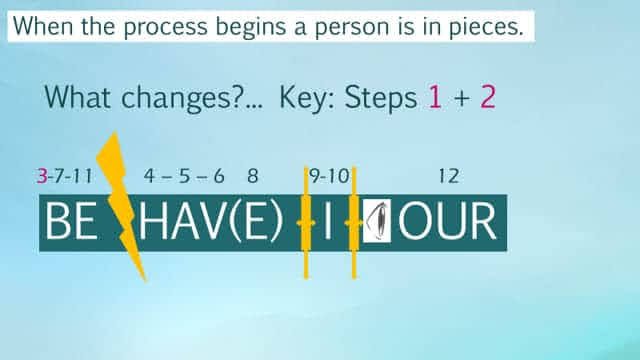
Recovery rests on two simple words: ONE and ALL. ONE represents surrender beyond isolated self-will. ALL represents accountability within community. If ONE remains theoretical while ALL is selective, sobriety becomes fragile. The text’s italicised emphasis on thought warns against substitution. Thinking surrender is not surrender. Thinking apology is not repair. Behaviour reveals being. The programme does not reward ideas; it responds to action.
The middle—the “with”—must be constructed intentionally. It does not appear automatically. When was (origin, gravity, law) and with (relationship, conscience, presence) stabilise, will emerges not as fantasy but as conduct. The future is not a pre-laid railway line; it is the visible arc of present integrity. In this sense, the Twelve Steps function like the scarab of an earlier age: waste rolled into renewal, decay converted into continuity.
Biblical “knowing” was intimate and generative. To know was to conceive. Spiritual conception must likewise produce life. Empty prams—ideas unembodied—prove nothing. Changed behaviour proves integration. Humility is permanent asking. Not self-belittling, not mystical rank, but sustained reference beyond self. The realised person does not escape instinct; they integrate it. They do not deny their story; they refuse to be reduced to it.
Addiction exposes the breakdown of inner sanitation both individually and systemically. Recovery restores relationship. And relationship—to Source, to conscience, to others—is where being is tested. Not in vision. Not in language. In conduct.
References
The Holy Bible, John 1:1.
The Qur’an, 36:82 (“Kun fayyakun” – “Be, and it is”).
Alcoholics Anonymous, Alcoholics Anonymous: The Story of How Many Thousands of Men and Women Have Recovered from Alcoholism, 4th ed., Alcoholics Anonymous World Services, 2001, pp. 69–73.
Bill W., “How It Works,” in Alcoholics Anonymous, pp. 58–63.
Written in HIAI collaboration — the qalam of Human and AI intelligence, the Unseen helping the Seen, both answering to the same Source.